 UP2 Slide (1)
UP2 Slide (1)References
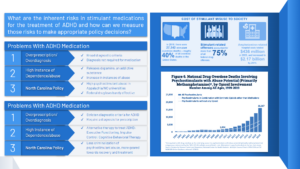
National Institute on Drug Abuse. (2022). Figure 6. Trends and statistics. [Graph]. Overdose death rates. Retrieved March 20, 2022 from https://nida.nih.gov/drug-topics/trends-statistics/overdose-death-rates.
Substance Abuse and Mental Health Services Administration. (2021). Cost of stimulant misuse to society. Treatment of Stimulant Use Disorders. [Digital infographic]. Evidence-Based Resource Guide Series. Retrieved March 24, 2022 from https://www.samhsa.gov/resource/ebp/treatment-stimulant-use-disorders.
Presentation Script:
While the majority of drug overdose deaths in the United States are attributed to the current opioid epidemic, an alarming portion of these deaths stem from the abuse of psychostimulants, according to Mattson et al. Given the reportedly-high volume of psychostimulant abuse in North Carolina, more stringent regulations on prescribing medication and a greater push for alternative methods of treating Attention Deficit Hyperactivity Disorder (ADHD) should be enacted to help curb the growing issue.
The majority of recently-published literature suggests that ADHD is overdiagnosed, which is likely a result of the broad criteria for ADHD. The Diagnostic and Statistical Manual of Mental Disorders describes ADHD as a pattern of inattentiveness, inability to plan, impulsivity, and the like. Moreover, most individuals treated for ADHD are given psychostimulants, according to Chan et al.. To make matters worse, North Carolina law does not require a diagnosis to attain a prescription for ADHD medication, which is widely believed to have inflated the distribution of prescription psychostimulants and instances of abuse. To curb overprescription, a formal ADHD diagnosis should be required.
Spencer et al. elaborate that Psychostimulants’ chemical makeup causes increases in pleasure, attentiveness, and motivation, which is why they are widely used in treating ADHD and is a reason for its abuse in high-stress settings. Given the high volume of prestigious universities in North Carolina, it is a hotspot for abuse and illegal distribution of prescription psychostimulants. North Carolina law classifies ADHD medications as Schedule II substances, meaning they require a prescription for use of any kind. Violation of Schedule II is a criminal offense, which, according to Chandler et al., is only “marginally effective,” in treating drug abuse. However, Chandler et al. highlight that recovery actions are far more effective at treating addiction than criminalization. Likewise, a change in North Carolina policy would accommodate this issue. Namely, decriminalization of psychostimulant use and implementation of a more rehabilitative, educational treatment.
Further, the overwhelmingly negative side effects of psychostimulant abuse outweigh the temporary enhancements in the mental acuity of the user. According to the American Psychiatric Association, behavioral therapy, such as cognitive-behavioral therapy, executive functioning therapy, and impulse control therapy are non-medicinal methods proven to be effective in treating ADHD without the negative side effects. Though behavioral therapy requires routine therapy sessions, the long-term benefits of learning to live with ADHD far exceed the inconvenience, as stated by Chan et al..
In sum, there are a variety of methods to treat the growing problem of psychostimulant abuse. Perhaps a combination of requiring a diagnosis to acquire prescription psychostimulants, rehabilitation to combat psychostimulant addiction, and exploration of behavioral therapies as the primary treatment for ADHD should be implemented. If shown to be effective in North Carolina, perhaps said methods may be applied to the entire United States in hopes to combat the growing problems of psychostimulant abuse.
Explication of Research:
While the majority of drug overdose deaths in the United States are attributed to the current opioid epidemic, an alarming portion of these deaths stem from the abuse of psychostimulants (Mattson et al., 2021, p. 205). Though opioid overdoses may claim more lives, the opioid epidemic casts a shadow on the imminent issues regarding abuse of Attention-Deficit Hyperactivity Disorder (ADHD) medication. Psychostimulants, while effective in treating ADHD, are also a heavy concern for recreational abuse (Chan et al., 2012, p. 37). Not only is ADHD over-diagnosed, but its highly-addictive psychostimulant medication also does not require a diagnosis, making it far too easy to acquire a prescription (Chan et al., 2012, p. 39). While psychostimulants are proven to be effective in treating the side-effects of ADHD (Faraone & Biederman, 2002, p. 69), the tolls that these medications have both on the developing brain and drug abuse far outweigh the benefits (Chan et al., 2012, p. 39). Since the inherent societal risks of psychostimulants outweigh the benefits, there is a need for stricter policy regarding the distribution of ADHD medication and a greater push for alternative methods of treating ADHD to combat the growing psychostimulant problem in North Carolina.
The majority of recently-published literature suggests that ADHD is overdiagnosed in the United States. The Diagnostic and Statistical Manual of Mental Disorders describes ADHD as a pattern of inattentiveness, inability to plan, impulsivity, and the like (American Psychiatric Association, 2013, p. 59). The broad nature of the disorder, wherein a simple attention issue can be mistaken as ADHD, leaves significant room for error when determining a diagnosis. This problem is prevalent when diagnosing children, where nearly 10% of elementary-aged children in the U.S. fit the criteria for ADHD, which is a significant increase from the 5% of diagnosed adults worldwide (Mahone & Denckla, 2017, p. 916). This means that some individuals “grow out” of their ADHD before adulthood, and others’ childlike behavior is mistaken for ADHD. In either case, Labeling ADHD as a disorder should require difficulty in living day-to-day life as a result of symptoms. In only these more severe cases psychostimulants should warrant a prescription. However, most individuals treated for ADHD are given psychostimulants, even those who exhibit mild symptoms (Chan et al., 2012, p. 39). To make matters worse, North Carolina law does not require a diagnosis to attain a prescription for ADHD medication, which is widely believed to have inflated the distribution of prescription psychostimulants and instances of abuse (Evans et al., 2010, p. 673).
To curb overprescription, a formal ADHD diagnosis should be required and the criteria for ADHD should be more strict. The requirement of a formal diagnosis would, in turn, prevent the prescription of ADHD without probable cause (a diagnosis) and force doctors to consider the severity of a patient’s symptoms prior to prescribing medication. Further, regulations should change to allow exclusively psychiatrists or psychologists to diagnose ADHD. This preventative measure ensures that a professional, versed in the field of mental illness, makes the decision of whether the drug is necessary, prior to a primary care doctor or pediatrician assessing whether the medication is safe for the patient.
The tolls of psychostimulants on both the brain and society outweigh the benefits provided to individuals taking psychostimulants. Psychostimulants cause the release of the chemical messenger (or neurotransmitter) dopamine, in excess, to the brain of the user. This chemical makeup causes increases in pleasure, attentiveness, and motivation in the user, which is why they are widely used in treating ADHD (Mahone & Denckla, 2017, p. 916-917). Further, the experienced pleasure and benefits to work ethic are reasons for its addiction and abuse in high-stress environments. Given the high volume of prestigious universities, North Carolina is a hotspot for abuse and illegal distribution of prescription psychostimulants (Mattson et al., 2021, p. 205). North Carolina law classifies ADHD medications as Schedule II substances, meaning they are both addictive and dangerous when taken in high doses and, consequently, require a prescription for use of any kind (Evans et al., 2010, p. 673). Violation of Schedule II is a criminal offense, which, is only “marginally effective,” (Chandler et al., 2017, p. 16) in treating drug abuse. However, the broad literature on drug abuse recovery claims that recovery actions are far more effective at treating addiction than criminalization.
Likewise, a change in North Carolina policy would accommodate the escalating issue of psychostimulant abuse. Namely, decriminalization of psychostimulant use and implementation of a more rehabilitative, educational treatment. This recovery would allow many affected individuals a means to sobriety without fear of punishment and without stigmas attached. Alternative methods of de-escalation of the psychostimulant problem are more prevalent now than ever, as the increasing popularity of ADHD medication contributed to an increase from 1,854 to 16,167 deaths from 2010 to 2019 in the U.S. (National Institute on Drug Abuse, 2022). These overwhelmingly negative impacts call for alternative methods of treatment for ADHD to deescalate the volume of prescribed psychostimulants.
Of the alternative methods to treat ADHD, the literature suggests that Behavioral therapy serves as an effective substitute for psychostimulants (Chan et al., 2012, p. 38). Further, the overwhelmingly negative side effects of psychostimulant abuse outweigh the temporary enhancements in the mental acuity of the user (Chan et al., 2012, p. 39). According to the American Psychiatric Association, behavioral therapy, such as cognitive-behavioral therapy, executive functioning therapy, and impulse control therapy are non-medicinal methods proven to be effective in treating ADHD without the negative side effects (American Psychiatric Association, 2017). These therapies, while not eliminating the symptoms of ADHD, teach necessary skills for living with ADHD, such as specific methods of planning and conditioning against impulsive and hyperactive behaviors. Though these behavioral therapies are effective to the majority of ADHD patients, they are not encompassing, so some individuals will still choose the route of medication. That is expected, as the purpose of pushing for alternatives to medication is to limit the unnecessary volume of psychostimulants, not to eliminate or stigmatize them completely. Though behavioral therapy requires routine therapy sessions, the long-term benefits of learning to live with ADHD far exceed the inconvenience (Chan et al. 2012, p. 39).
In sum, there are a variety of methods to treat the growing problem of psychostimulant abuse. Perhaps a combination of requiring a diagnosis to acquire prescription psychostimulants, rehabilitation to combat psychostimulant addiction, and exploration of behavioral therapies as the primary treatment for ADHD should be implemented. While requiring a diagnosis would ensure treatment for more moderate to severe cases of ADHD, thus limiting the inflation of distributed psychostimulants, behavioral therapies would still allow treatment for more mild cases and serve as an equally effective alternative. If shown to be effective in North Carolina, perhaps said methods may be applied to the entire United States in hopes to combat the growing problems of psychostimulant abuse.
References
American Psychiatric Association. (2013). Neurodevelopmental disorders. Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596.dsm05.
American Psychiatric Association. (2017). What is Cognitive Behavioral Therapy? PTSD Guideline. https://www.apa.org/ptsd-guideline/patients-and-families/cognitive-behavioral.
Berke, J., & Hyman, S. (2000). Addiction, dopamine, and the review molecular mechanisms of memory alertness and produce a sense of well-being. Neuron, 25, 515–532. https://www.cell.com/neuron/pdf/S0896-6273(00)81056-9.pdf.
Chan, J. Y. C., Dennis, T. A., & MacLeod, M. A. (2012). The over-prescription of Ritalin for suspected cases of ADHD. Uottawa.ca, 2(2), 35–40. https://doi.org/http://hdl.handle.net/10393/34386.
Chandler, M. J., Locke, D. E., Crook, J. E., Fields, J. A., Ball, C. T., Phatak, V. S., Dean, P. M., Morris, M., & Smith, G. E. (2019). Comparative Effectiveness of Behavioral Interventions on Quality of Life for Older Adults With Mild Cognitive Impairment: A Randomized Clinical Trial. JAMA network open, 2(5), 1–18. https://doi.org/10.1001/jamanetworkopen.2019.3016
Evans, W. N., Morrill, M.S., & Parente, S.T. (2010). Measuring inappropriate medical diagnosis and treatment in survey data: The case of ADHD among school-age children. Journal of Health Economics, 29(5), 657-673. https://doi.org/10.1016/j.jhealeco.2010.07.005.
Faraone, S. V., & Biederman, J. (2002). Efficacy of Adderall for Attention-Deficit/Hyperactivity Disorder: a meta-analysis. Journal of Attention Disorders, 6(2), 69–75. https://doi.org/10.1177/108705470200600203.
Mahone, E. M., & Denckla, M. B. (2017). Attention-Deficit/Hyperactivity Disorder: A Historical Neuropsychological Perspective. Journal of the International Neuropsychological Society: JINS, 23(9-10), 916–929. https://doi.org/10.1017/S1355617717000807.
Mattson, C. L., Tanz, L. J., Quinn, K., Kariisa, M., Patel, P., & Davis, N. L. (2021). Trends and geographic patterns in drug and synthetic opioid overdose deaths — United States, 2013–2019. MMWR. Morbidity and Mortality Weekly Report, 70(6), 202–207. https://doi.org/10.15585/mmwr.mm7006a4.
National Institute on Drug Abuse. (2022). Figure 6. Trends and statistics. [Graph]. Overdose death rates. Retrieved March 20, 2022 from https://nida.nih.gov/drug-topics/trends-statistics/overdose-death-rates.
Spencer, T. J., Brown, A., Seidman, L. J., Valera, E. M., Makris, N., Lomedico, A., Faraone, S. V., & Biederman, J. (2013). Effect of psychostimulants on brain structure and function in ADHD. The Journal of Clinical Psychiatry, 74(9), 902–917. https://doi.org/10.4088/jcp.12r08287.