The Autism Community in Action. Autism statistics & cost. Retrieved March 24, 2022, from https://tacanow.org/autism-statistics/.
Script
Autism Spectrum Disorder, or ASD, is a neurodevelopmental disorder that includes many symptoms and well-known disorders, like Asperger’s syndrome. Very little is known about the severity of autism and its relation to socioeconomic status, or SES. I will discuss some factors that may be related to the severity of autism and provide some strategies to improve equity in gaining autism healthcare in North Carolina.
When looking for SES factors related to autism severity, I looked at race and obesity. The first factor, race, is a known factor that affects the diagnosis of autism. One study conducted in North Carolina showed that African American students were more likely to receive a primary diagnosis of intellectual disability over ASD than their White counterparts (Howard et al., 2021), and on average were diagnosed with ASD at an older age (Emerson et al., 2016). This suggests that physicians are not familiar with autistic behavior more common to certain races or are biased in diagnosis. Diagnosis age is crucial to receiving timely treatment; the treatment may not be as effective if received later, causing more severe symptoms. As a result, this barrier to healthcare may cause a biologically unrelated correlation between race and ASD severity.
The second factor, obesity, is very common in children with ASD and other developmental disorders. In the U.S., children with ASD are 1.57 times more likely to be overweight, and children with severe ASD symptoms are 1.7 times more likely to be overweight than those with mild symptoms (Healy et al., 2019; Levy et al., 2019). Obesity is also known to be linked to SES—children of lower SES are generally more at risk for obesity (McLaren, 2007). It is therefore possible that the higher risk of obesity in children with severe autistic symptoms is because children of lower SES have more severe symptoms and are more at risk for obesity, but more research is needed to support this.
As to the inequity in gaining healthcare for ASD individuals, there are policies that can help. All states must cover medically necessary therapies that treat ASD for children with Medicaid. The mandate also covers many private health plans, which has helped many families cut costs. However, problems like poor coverage of healthcare providers and insurance companies denying reimbursement have created barriers (Baller et al., 2016). To make the mandate more effective, we could loosen the requirements for private practices to treat ASD to increase the supply of services. We could also recruit and train schoolteachers to identify autistic behavior in the classroom to promote earlier diagnosis, all of which are in the interest of public health.
Explication of research
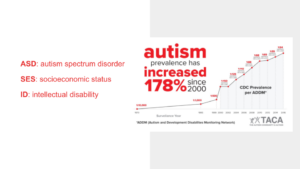
Autism Spectrum Disorder (ASD) is a multifactorial neurodevelopmental disorder that encompasses many symptoms and well-known disorders, including Asperger’s syndrome. The number of diagnosed cases of ASD has been on the rise (CDC, 2020, 2021), and science has yet to reveal the cause(s) behind the drastic increase. In the U.S. alone, numbers rose from one in 1000 births in 1995 to one in 59 births in 2018 (CDC, 2021).
Past studies have revealed correlations between the prevalence of ASD and socioeconomic factors such as race and family income, and hint to gaps in healthcare access among different populations. In contrast, relatively few studies focus on the severity of autism and its relation to socioeconomic factors/status (SES), likely due to the complexity of the disorder itself. Autism is suspected to be a genetically inheritable disorder, but many non-genetic factors come into play (Muhle et al., 2004), influencing severity of symptoms. It is possible to identify some of these non-genetic factors. Ultimately, this explication aims to highlight new research directions for ASD and to formulate possible solutions to improving equity in healthcare for ASD individuals in the state of North Carolina.
In one study conducted in North Carolina, researchers explored the relationship between race and economic advantage, and the primary classifications of ID or ASD in school children. Though ID and ASD were examined separately, the researchers did note that ASD and ID can cooccur, and they found that African American students were more likely to receive a primary classification of ID than White students. Furthermore, there was an even stronger correlation between household income and diagnosis of ID and ASD: as the log of median income increased, diagnosis of ASD increased, whereas the proportion of ID students decreased (Howard et al., 2021). This could be an indication of SES factors correlating to the diagnosis of autism severity, or misdiagnosis of developmental disorders in general, within North Carolina.
Misdiagnosis or delay in diagnosis itself also contributes to autism severity. In general, children with moderate autism were diagnosed with autism earlier than children with mild or severe autism (Emerson et al., 2016, pg. 131). Contrary to popular belief, children of ethnic minority were generally diagnosed at an earlier age than Caucasian children. This could have resulted from cultural differences in family dynamics, in which ethnicities with more family-oriented cultures sought diagnosis earlier. However, children born into African American households with a consistent source of care (CSC) were diagnosed later in comparison to Caucasian households with CSC, indicating the possibility that physician diagnosis is biased based on race (Emerson et al., 2016, pg. 134). Another study showed a similar bias: “African American children required 3 times the number of visits over a period 3 times as long as White children before being diagnosed with an autism” (Mandell et al., 2002; Travers et al., 2013). Age of diagnosis is crucial for timely treatment, and later diagnosis age could result in treatment becoming less effective in improving the severity of autism. Yet widespread, prolonged or biased diagnoses leave ASD children of racial minorities at risk for not receiving prompt treatment. Physicians may also be less familiar with autistic behaviors associated with African American children, as research has shown certain autistic behaviors are more common in Caucasian children and vice versa (Becerra et al., 2014), further exacerbating the problem. These barriers to healthcare could in turn cause a biologically unrelated correlation between race and autism severity (Emerson et al., 2016) that current policies and support systems do not address.
Another factor related to SES and autism worth noting is obesity. A health condition commonly associated with lower family income and SES in developed countries (McLaren, 2007), obesity is also prevalent in children with ASD or developmental delays. Levy et al. (2019) showed that in the U.S., children with ASD were 1.57 times more likely than the general population controls to be overweight; within the ASD population, children with severe ASD symptoms were 1.7 times more likely to be classified as overweight than those with mild ASD symptoms (Healy et al., 2019). Child obesity is known to be linked to SES as well: children of lower SES generally have higher levels of obesity and prevalence of obesity is higher in African American children when compared to Caucasian children (Strauss & Knight, 1999). It is therefore possible that the higher risk of obesity in children with severe autistic symptoms is because children of lower SES have more severe symptoms and are more at risk for obesity, but more research would be required to support this speculation. Low-income households with an autistic child would likely experience greater difficulty in obtaining quality autism healthcare and nutrition, which may contribute to more severe autistic symptoms as well.
Although available data all seem to hint to a link between severity level in autism and socioeconomic status, few show correlation or causation. Regardless, present data has shown promise within the field for new research directions. In addition, the alarming presence of bias in autism diagnosis related to SES also call for a need to implement strategies to improve healthcare equity for autistic households, as autism has a growing worldwide prevalence (Elsabbagh et al., 2012). In the U.S., a nationwide mandate that compels states to cover medically necessary therapies that treat ASD for children with Medicaid has helped many families cut out-of-cut spending, but many problems arise with the mandate. Many healthcare providers simply do not have enough certified personnel to perform ASD treatment across their networks, and some private practices have been forced to close due to the introduction of stringent certification rules for ASD treatment professionals, creating a shortage in supply. Specific private insurance companies are also required to cover ASD treatments, yet many take advantage of loopholes in the law to deny reimbursement (Baller et al., 2016). North Carolina is known to have an adequate service system for young children with ASD (Thomas et al., 2007), but there is an observed primary diagnosis difference between rural and urban counties, suggesting that there are differences in quantity and quality of healthcare based on geographical location. Frustrations that other states experience may apply to North Carolina, which could be partially addressed by updating insurance mandate policies. To increase supply, local governments could collaborate with qualified ASD institutions to create ASD treatment certification, which would allow capable medical professionals that may not meet the education qualifications to obtain an alternative certification for opening their practices. Improving wording in specific laws could curb private insurance companies from exploiting loose wording as well. The increase in supply of services may not apply to rural counties that already lack from a deficit of general healthcare, so implementing additional measures to support and promote better healthcare is necessary as well. Local communities could raise awareness of ASD through educational events and teach residents to recognize potential autistic behavior. Local hospitals or private practices could work with school districts to promote earlier diagnosis by recruiting and training schoolteachers to identify autistic behavior in the classroom. These strategies may not eradicate inequity in ASD healthcare in North Carolina—they are meant to complement existing systems—but they would likely improve racial- or SES-related barriers to health. The lack of healthcare in rural North Carolina is a complicated issue that affects populations far beyond people on the spectrum.
With the rising prevalence of ASD, it would be in the interest of public health to provide effective and equitable healthcare for autistic patients and families. Research should focus on identifying barriers in healthcare, especially regarding severity of autism, and local governments and communities should play a larger role in supporting the ASD population in their pursuit of health and happiness.
References
Baller, J.B., Barry, C.L., Shea, K., Walker, M.M., Ouellette, R., & Mandell, D.S. (2016) Assessing early implementation of state autism insurance mandates. Autism, 20(7), 796 –807. https://doi.org/10.1177/1362361315605972.
Becerra, T. A., von Ehrenstein, O. S., Heck, J. E., Olsen, J., Arah, O.A., Jeste, S. S., et al. (2014) Autism spectrum disorders and race, ethnicity, and nativity: a population-based study. Pediatrics, 134(1), e63–e71. https://doi.org/10.1542/peds.2013-3928.
CDC, U.S. Department of Health and Human Services. (2020). Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years —Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016 (Morbidity and Mortality Weekly Report, Vol. 69, No. 4). Centers for Disease Control and Prevention. https://www.cdc.gov/mmwr/volumes/69/ss/ss6904a1.htm
CDC, U.S. Department of Health and Human Services. (2021). Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years —Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018 (Morbidity and Mortality Weekly Report, Vol. 70, No. 11). Centers for Disease Control and Prevention. https://www.cdc.gov/mmwr/volumes/69/ss/ss6904a1.htm
Elsabbagh, M., Divan, G., Koh, Y., Kim, Y.S., Kauchali, S., Montiel-Nava, C.M.C, Patel, V., Paula, C.S., Wang, C., Yasamy, M.T., & Fombonne, E. (2012) Global prevalence of autism and other pervasive developmental disorders. Autism Research, 5(3), 160–179. https://doi.org/10.1002/aur.239.
Emerson, N.D., Morrell, H.E.R., & Neece, C. (2016) Predictors of age of diagnosis for children with autism spectrum disorder: the role of a consistent source of medical care, race, and condition severity. Journal of Autism and Developmental Disorders, 46(1),127–138. https://doi/org/10.1007/s10803-015-2555-x.
Healy, S., Aigner, C.J., & Haegele, J.A. (2019) Prevalence of overweight and obesity among US youth with autism spectrum disorder. Autism, 23(4), 1046–1050. https://doi.org/10.1177/1362361318791817.
Howard, J., Copelan D, J.N., Gifford, E.J., Lawson, J., Bai, Y., Heilbron, N., & Maslow, G. (2021) Brief report: classifying rates of students with autism and intellectual disability in north carolina: roles of race and economic disadvantage. Journal of Autism and Developmental Disorders, 51(1), 307–314. https://doi.org/10.1007/s10803-020-04527-y.
Kim, E.T., Franz, L., Fannin, D.K., Howard, J., & Maslow, G. (2021) Educational classifications of autism spectrum disorder and intellectual disability among school-aged children in north carolina: associations with race, rurality, and resource availability. Autism Research, 14(5), 1046–1060. https://doi.org/10.1002/aur.2492.
Mandell, D.S., Listerud, J., Levy, S.E., & Pinto-Martin, J.A. (2002) Race differences in the age at diagnosis among medicaid-eligible children with autism. Journal of American Academy of Child and Adolescent Psychiatry, 41(12),1447-1453. https://doi.org/10.1097/00004583-200212000-00016.
Levy, S.E., Pinto-Martin, J.A., Bradley, C.B., Chittams, J., Johnson, S.L., Pandey, J., Pomykacz, A., Ramirez, A., Reynolds, A.,Rubenstein, E., Schieve, L.A., Shapira, S.K., Thompson, A., Young, L., & Kral, T.V.E. (2019) Relationship of weight outcomes, co-occurring conditions, and severity of autism spectrum disorder in the study to explore early development. The Journal Of Pediatrics, 205, 202-209. https://doi.org10.1016/j.jpeds.2018.09.003.
McLaren, L. (2007) Socioeconomic Status and Obesity. Epidemiologic Reviews, 29, 29-48. https://doi.org/10.1093/epirev/mxm001.
Muhle, R., Trentacoste, S.V., & Rapin, I. (2004) The Genetics of Autism. Pediatrics, 113(5), e472–e486. https://doi.org/10.1542/peds.113.5.e472.
Strauss, R.S., & Knight, J. (1999) Influence of the Home Environment on the Development of Obesity in Children. Pediatrics, 103(6), e85, 1-8. https://doi.org/10.1542/peds.103.6.e85.
Thomas, K.C., Ellis, A.R., McLaurin, C., Daniels, J., & Morrissey, J.P. (2007) Access to care for autism-related services. Journal of Autism and Developmental Disorders, 37(10), 1902–1912. https://doi.org/10.1007/s10803-006-0323-7.
Travers, J.C., Tincani, M., & Krezmien, M.P. (2013) A multiyear national profile of racial disparity in autism identification. The Journal of Special Education, 47(1), 41-49. https://doi.org/10.1177/0022466911416247.
Featured image source
Rudy, L.J. (2021, November 02) Symptoms of autism in girls—autism in girls may look different from autism in boys. Verywell Health. Retrieved March 24, 2022, fromhttps://www.verywellhealth.com/signs-of-autism-in-girls-260304.