The Roe v. Wade decision derived a right to abortion from the 14th Amendment’s right to privacy. The Dobbs decision decided against this previous ruling, the Supreme Court ruling that the federal government cannot guarantee access to abortion under this protection. It is now a “permittance:” up to the states to either limit or guarantee, or Congress to federally guarantee or limit with the passage of new laws. I seek to explore how abortion is remembered as a right within American society, and how that did or did not affect the lack of federal legislation guaranteeing it. This has implications for other Supreme Court-derived rights as well, such as gay marriage, and the re-implication of abortion laws in states that never repealed them following Roe v. Wade.
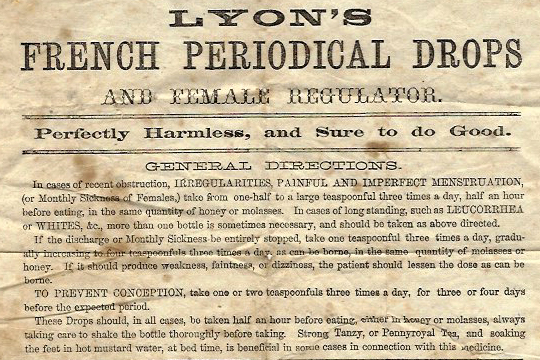
Advertisement for an abortifacient dating from the late 19th to early 20th century. “Curing female irregularities” was a common euphemism for abortion in this time period. (WKU Libraries)
Rights and Permittances: The Public Perception of Abortion in Shaping Legislation
At the United States’ inception, abortion was not seen as a right, but was regularly practiced. Inheriting from the British legal tradition, abortion was not considered a crime so long as it was performed prior to quickening – that is, prior to the mother being able to feel movement in the womb, typically occurring at 16 to 20 weeks into a pregnancy. By the mid-19th century, abortion was legal in 21 out of 33 states; in places where it was a crime, women were rarely prosecuted for it. This might strike modern Americans as surprising; indeed, pro-life policies are often associated with tradition, with the Christian religion that arrived on American soil with the very first colonists, an ancient thing for such a young country as the United States.
Scientific Progress and the Perception of Life
Scientific progress lead to the revelation that quickening is a fairly arbitrary method of determining life; it became known that a fetus gradually grows from a fertilized egg into an infant. Physicians led a movement to ban abortion on the grounds of a scientific definition of human life, and a desire to uphold the Hippocratic Oath. They had mixed success. On the one hand, efforts peaking in the in the Reconstruction Era, led by such figures as the controversial Horatio Storer and Anthony Comstock of Comstock Law fame, resulted in abortion being a felony in every state by the year 1900. Confounding this, however, were new public attitudes surrounding the topic developing. New ways of thinking about women’s health resulted in an increased demand for access to both contraceptives and abortion. Margaret Sanger’s American Birth Control League was founded in 1921, under the belief that the health of women, the families they raise, and thus society at large was greatly benefitted by women being able to control when and how many children to bear. This viewpoint, which combined views of both eugenics and feminism popular during this era, was not shared by all. The feminist line of thought in particular has not always been so uniform as might be imagined in the mind of the public. Indeed, of the Reconstruction Era feminists, many, such as Susan B. Anthony and Elizabeth Stanton, were opposed to abortion in the sense that it was a “undesirable necessity forced upon women by thoughtless men” (Mohr). Later feminists, namely those of the second-wave generation beginning in the 1960s, took a firm stance on abortion being an important aspect of female liberation, a position that has taken hold in the popular American memory as one strongly linked to feminism as a whole.
Bans advance in the early 20th century, by the 1960s abortion is illegal in most states. During this time…
Were abortions still practiced?
Were laws enforced?
Did women feel entitled to an abortion or not?
Which groups were pro-abortion? Which groups were anti-abortion? (make exceptional note of women’s political organization i.e. early vs later feminists, Sanger and early 20th century eugenicists, etc)
Roe v. Wade: A Right Codified in Law and Memory
Roe v. Wade derives an explicit right to an abortion from the Fifteenth Amendment. Since then, abortion is more and more thought of as a “right” in the minds of many Americans. A few remember the circumstances of the case and note that it is on legally shaky ground. Perhaps a good point to bring up the national approval rating on abortion legality in 1973 to present day (<50% to >50%). Link the memory of abortion as a right to the lack of legislative effort on actually federally creating that right during those 50 years.
Was it never a right, always a right, or something in-between?
The Dobbs ruling asks: “How does a right to privacy mean you can’t ban abortion? We ban all sorts of things done in private.” Now abortion is a legal permittance, up to the states to allow or guarantee, or federal legislation doing the same. The memory of abortions role in society is currently divided among different factions, philosophies, faiths, and personal beliefs. The Dobbs decision, a mere ruling on the nature of the US Constitution, has become a flashpoint for mutually exclusive thoughts on what constitutes a human, if not a legal right. i.e. note that many pro-life groups celebrate the victory as divine justice and not a correction of a previous legal mistake, and how pro-choicers adopt rhetoric of a fundamental human right being infringed, a right that if not deriving from the Constitution, is innate.
To learn more about the individual impact of the (de)legalization of abortion, Dr. Meera Shah shares intimate stories of individuals who have gotten abortions for all types of reasons in her novel. Dr. Shah is an Indian American abortion provider who discovered that many people have gotten an abortion in their lifetime but kept it a secret because of stigmas (Shah, 2020). She aims to take down this stigma by humanizing abortions. Through storytelling, individuals can provide more compassion to such a nuanced and divisive topic. After all, 1 in 4 women in America has received an abortion in their lifetime (Abortion is a Common Experience, 2017). Storytelling has the ability to change the narrative and memory around abortion in America. Abortion is not just political, but an everyday human issue. The stories range tremendously, meaning that everyone should be able to empathize with their experiences. Hearing these stories can help reshape society’s collective memory of abortion.
In Chapter 1, Sara is living in a cramped apartment with her partner and his children. They were already financially struggling when she realized she was pregnant. Sara was not sure if she wanted to be a mother, but getting pregnant was a confirmation that she did want to have kids one day, but this was not the day. In Texas, Sara was required to have an ultrasound and wait for 24 hours. Sara had already taken the time to make this decision confidently and felt tortured by the waiting period. Ironically enough, the Texas Rifle Association did not require any waiting period. After her abortion, she stayed with her partner who would end up getting arrested for physically abusing her. She ended up leaving the state to escape her relationship. She is glad that she had an abortion so she is not permanently tied to him.
In Chapter 3, Paige is a junior at the University of Michigan in 1972. Back then, there was little to no discussion of contraceptives. While she typically used a diaphragm, she didn’t use it once and tried to shake the sperm out of her. She got pregnant by her then-boyfriend. She knew she needed to finish college and graduate so having a baby was not an option. In 1972, Roe v Wade had not passed yet. Paige had to leave the state to go to New York for an abortion. Paige borrowed $200 from a neighbor (equivalent to $1200 today). She was immediately relieved after the procedure was done like she had gotten her life back, especially as a young woman. Paige would get pregnant again in 1975. This time, she considered keeping the child but decided she didn’t want to be a single mother and knew she couldn’t count on the father of the child. Her experience was not as pleasant the second time as she had a “horrible human being” of a doctor. Unlike her first pregnancy, sometimes she wonders what type of human her second pregnancy could have been. She doesn’t regret her decision but regrets that her birth control failed.
In Chapter 5, Mary is a Vietnamese American in her early 20s. She lives in NYC with her husband when she finds out she’s pregnant despite using condoms. When she was 26 weeks pregnant, her doctor tells her that the baby’s heart stopped beating and they would need to induce her labor. Her first pregnancy ended in a stillborn baby. She would go on to have a healthy son. Then, she was pregnant for the third time in her late 30s. She was in “geriatric” territory and opted for genetic testing, where she learned that her baby had Patau syndrome. Only 10% of babies with Patau make it past their first year and those who do face major health concerns. Mary wanted to stay pregnant and miscarry, but the doctor said there was still a good chance she would have to deliver. Sicken with grief, she chose to get an abortion, knowing that she wanted to have another baby. Now Mary is a mother to two young boys, and she says that her losses provided her with more gratitude for being a parent.
In a Buzzfeed article, Lieberman (2022) shares the story of Oliver, a trans man, who becomes pregnant. He chose to get an abortion because he was already struggling to support himself and knew that having an abortion was the right answer. Oliver’s experience is important to share when it comes to advocating for gender-inclusive language and adequate support for trans people regarding abortion rights. His story provides a partial memory of a larger abortion narrative. Often, people remember abortion as a women’s issue but by hearing individual stories of trans pregnant people, we can start to change our memory of abortion to a health issue that affects all genders.
In conclusion, each of these individuals’ stories is extremely unique to their circumstances, especially given race, class, age, and other factors. There is no one-size-fits-all approach when deciding to end a pregnancy. Each of these individuals chose to publicize their personal stories in hopes of helping American society better understand abortion as a human experience. Their stories became usable in shaping collective memory. Moreover, in many of these stories, there were obstacles to receiving appropriate health care, adding unpredictability to the memory of abortion rights. Having this unpredictable memory of inaccessibility is crucial to advancing abortion rights. Lastly, each individual felt many emotions of grief, relief, and loss after having an abortion as anyone would when they make a life-changing decision. Storytelling provides an avenue to process this experience while sharing it with a larger audience, thus serving as a processual memory. Publicizing a vulnerable moment like this gives these individuals the strength to further understand their emotions while also challenging a greater narrative of collective memory that fails to recognize the nuances and complexity of abortions.
A pro-choice protester in Denver holds up bloody wire coat hangers after the overturning of Roe v. Wade, 2022. (Jason Connolly/AFP via Getty Images)
A ubiquitous symbol in modern pro-choice protests, the coat hanger is a painful reminder of the extreme measures American women were forced to take to preserve their bodily autonomy before the landmark 1973 Roe v. Wade ruling. In 2022, just before the case’s 50th anniversary, Roe v. Wade was overturned, in a culmination of decades of mounting threats to reproductive rights; the resolution led to a cascade of trigger laws in conservative states limiting or outright banning abortion, which now define the post-Roe landscape. As in-clinic abortion becomes inaccessible to more and more Americans, many are turning towards DIY abortion as an alternative, unearthing cultural memories of a pre-Roe world in the process.
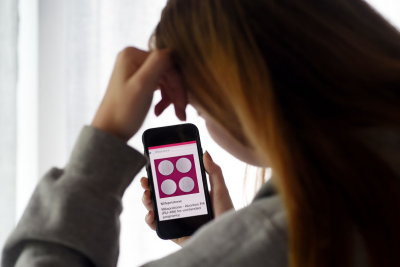
DIY abortions often conjure grisly images of agonizing pain and dangerous infections, an enduring partial memory strengthened by the prevalence of material artifacts and symbols, such as the infamous coat hanger that has been mobilized in support of reproductive rights around the world. However, today’s DIY abortions most frequently take the form of two pills: mifepristone and misoprostol, which induce miscarriages and are typically prescribed by doctors. Although the two-pill procedure is FDA-approved for up to 10 weeks [1], with a 0.31% serious complication rate [2] and 95% effectiveness [3], obtaining the pill still poses a barrier to many women—abortion networks and funds, such as Dutch organization Women on Web, usually prioritize locations that outlaw abortion entirely [4], leaving women in states that have seen abortion clinics becoming few and restrictions being added effectively stranded.
“This has to look like a miscarriage.”
“I cry and pray every night that the Lord take this child from me somehow.”
“Please, I am out of options.”
These messages sent to abortion networks [4] reflect a universal sense of desperation, spanning class, marital status, age, and time. Mirroring the pre-Roe era, the barriers faced by these women are startlingly similar to the ones being built today: with legal abortions only available in a few major cities [5], women who were in other states and unable to travel also found themselves physically stranded, unable to safely terminate their pregnancies.
Both in the pre-and post-Roe era, we find that those seeking abortion do not give up, but instead turn to increasingly dangerous methods. Turpentine is just one recurring motif—women drink it, insert cotton balls soaked with it into their vaginas, and inject it into their abdomens [4]. Multiple current-day and historical cases chronicle the physical last resorts taken by desperate women in the absence of safe methods, including the insertion of objects like the infamous wire coat hanger and even instances of women shooting themselves in the stomach.
In response to these lethal methods and official regulations that ignored women’s plight, the 1960s saw vernacular pushback in the form of underground abortion groups, like the Chicago-based Jane Collective, which provided safe abortion services to roughly 11,000 women between 1969 and 1973 [6]. In contrast to today’s preferred two-pill procedure, the dilation and curettage procedures primarily used then were surgical, involving the physical removal of tissue from the uterus. While the women performing these procedures were often untrained, and health risks remained, no deaths were ever associated with the procedures that Jane performed [6]. The testimonials of Jane volunteers form a collective portrait of the pre-Roe era: abortions shrouded in secrecy and disguised with coded language, paired with a sense of warlike urgency.
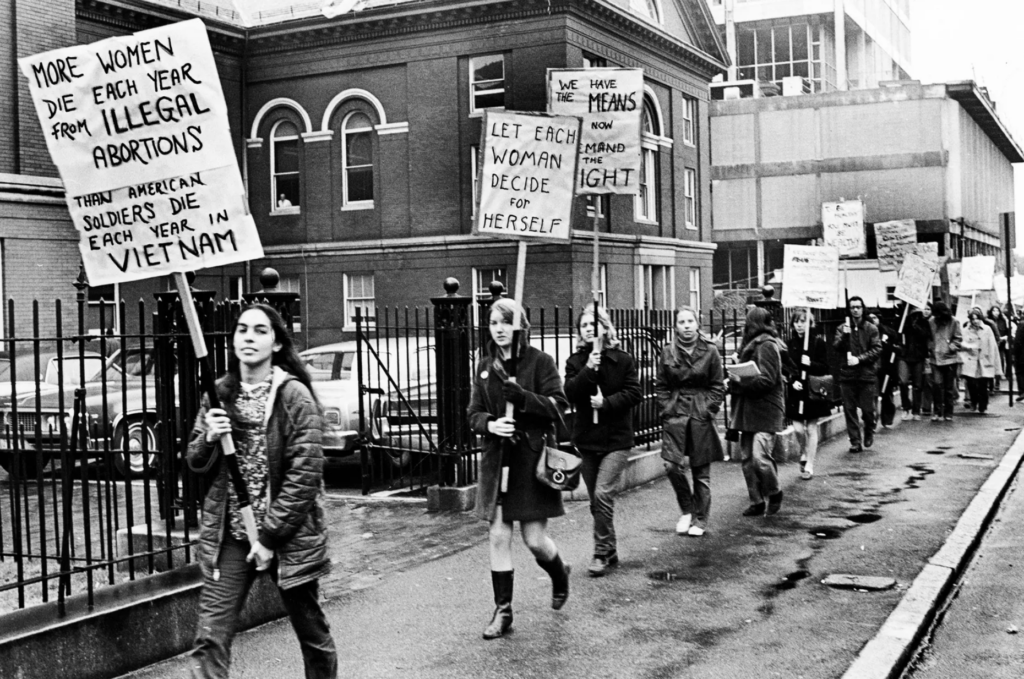
Women in Boston protesting abortion restrictions before Roe v. Wade, 1969. (Getty Images)
After Roe v. Wade was passed in 1973, these groups disbanded as the need decreased, and with the advent of safe, legal abortions, recorded deaths due to self-induced abortion complications dropped dramatically from over 200 to just 3 per year [4]. The anti-abortion historical narrative pushed by official memory-makers often obscures these darker aspects of history, but vernacular memory does not forget—preserved in books, films, and firsthand accounts, today’s pushback is especially prevalent on social media, where activists share abortion resources and guidance with stranded women.
In the post-Roe present, reproductive rights continue to be threatened. In several states, notably South Carolina and Nevada, laws criminalize those pursuing self-induced abortions, and have resulted in women being charged with aggravated assault [4] or murder [7] after seeking medical treatment for complications.
At the time of this article’s publication, the Supreme Court is currently determining whether mifepristone, one of the pills in the two-pill procedure, should remain on the market; its removal would mean a decrease in the effectiveness of pill abortions, and further render safe abortions inaccessible [8]. The anti-abortion argument for the restriction of the abortion pill also demonstrates the partial aspect of collective memory and how the same cultural memory can be mobilized for different causes—the dominance of the coat hanger as the pinnacle of DIY abortion reinforces the idea that all self-induced abortion methods put women’s lives at significant risk, despite the two-pill method’s proven safety over other DIY methods [2]. In reality, the pre-Roe era indicates that when safe abortion is inaccessible, dangerous methods like coat hanger abortions become many women’s only option.
As the post-Roe era landscape becomes clearer and more defined, the pre-Roe era and cultural memory of underground and self-induced abortions are a significant resource for indicating what the future may yield. The history of DIY abortion, specifically, is an important site of cultural reflection, functioning as a reminder of what a post-Roe world might look like—the processual and partial aspects of memory make it easy to forget why exactly Roe v. Wade was so significant in women’s lives and the widespread suffering that abortion bans brought. The pre-Roe era demonstrates a fundamental truth of abortion restrictions: women will preserve their bodily autonomy at any cost, and in a post-Roe landscape, it is not simply a matter of whether an individual seeking an abortion will get one, but the method by which they do it.
A medical bed sits in an abortion clinic located in Tulsa, Oklahoma that was active before the overturning of Roe v. Wade in 2022 [1].
Abortion has been a very controversial and widely discussed topic in the United States for a long time now. Since the Roe v. Wade decision in 1973 that made abortion practices legal in the United States, the medical procedures involved in performing abortions have been drastically improved. Before they were legalized, many women had to perform DIY processes for abortions which were very unsafe and would put the health of the women at risk. With the advancements in medical technology, today there are many ways to perform safe abortions. Abortion clinics are open to the public and many new techniques are still being developed, such as new pills and chemical abortions that will make the process even more convenient. However, future techniques and procedures being developed and improved upon are at risk of not happening with the recent overruling of the Roe v. Wade case. The article aims to provide a description of the terminology associated with abortion procedures, the improvements made in the medical field of abortion, the memory associated with abortion procedures, and what will be impacted going into the future after the recent decision by the Supreme Court.
Early abortion techniques were very unconventional because society at large did not accept abortion as a common practice, so women had to find ways to perform the procedure themselves. In North America between the 1600s and 1700s, tribal groups would use black root and cedar root as abortifacient agents [5]. Even going a little bit further into history around the 1970s after the passing of the Hyde Amendment, women would still have to use illegal underground abortion centers to have these procedures [5]. These institutions would often have people who were medically qualified. This could then lead to infections or cases of severe bleeding that would put the health of the women at severe risk or possibly even lead to their death. However, after the Roe v. Wade case, more resources and research could go into medical technology that could be utilized to improve abortion procedures.
One of the current abortion techniques is clinic abortions, sometimes called surgical abortions, which require a visit to an abortion clinic or another medical facility. The most common type of clinic abortion is known as a vacuum aspiration, which uses gentle suction to empty the uterus and occurs 14-16 weeks after the women’s last period [2]. This typically occurs in the first trimester so if you are in the second trimester, a Dilation and Evacuation technique is most likely required. D&E also uses suction with various medical tools to empty the uterus with 16 weeks past the last period [2]. The other type of procedure is Dilation and Extraction, which is only used if there are major problems with the fetus or the mother, which sedates the mother and removes the fetus [4]. Before the procedure takes place, the patient is required to contact the health professional for instructions such as fasting before the procedure [4]. There are many steps prior to the treatment that must take place such as blood tests, physical examinations, looking for infections, and other information given to the patient to disclose all the facts regarding the process [4]. During the procedure there are also different medications given for pain management such as ibuprofen and anesthesia to numb the cervix [4]. Though the other type of abortion technique is easier, clinic abortions are often used because they work 99 out of 100 times and they only take 5-10 minutes instead of 24 hours [2].
The other type of abortion procedure is a medical abortion, which takes place by ingesting a pill that extracts the fetus from the patient’s home. One pill that is currently used is mifepristone, which blocks progesterone, and this hormone is needed to continue the process of the pregnancy. It is used up to ten weeks since last period and about 1-2 days later, misoprostol is used to create a miscarriage, which in turn terminates the pregnancy. At the doctor’s office you take 200 mgs of mifepristone and at home you take 800 mgs, or four pills, of misoprostol [6]. These pills can cause short term side effects like bleeding, nausea, vomiting, and chills, but there is no evidence of long-term effects [6]. Looking to the future of new methods for abortions, the TelAbortion Project is being developed. The goal is to bring these prescriptions like mifepristone and misoprostol directly to the patient’s home or through the mail after consulting with their doctor and watching a video [3]. There was a test in 2017 with certain pregnant women who had videoconferences with different physicians for this project, and out of the 60 women who completed the project, 59 of the participants were satisfied [3]. This project is even more beneficial coming off the Covid-19 pandemic because it is safer and easier than ever with advancements in technology to avoid going to the clinic. However, with the overturning of Roe v. Wade, this makes this process impossible in states where they have abortion illegal, so the future of the TelAbortion Project and other new abortion procedures remains unknown.
Advancements in medical technology as well as abortions being made legal in 1973 have led to vast improvements in abortion medical procedures. However, it is also very interesting that these improvements show how processual and unpredictable the memory of abortions are in the United States. Science and technology are very processual because new things are being discovered as we go in the future so the way we view past methods of procedures are forever adapting. It is unpredictable because opinions of people’s view on abortions have changed in different periods of time. There have been points where abortions have been illegal and there have been points where it has been legal, and we are once again at a point where it has been deemed illegal by the federal government. This directly correlates with the medical aspect of abortions because if it is once again federally illegal, less resources will be put into technology and less advancements can be made in the field. With the everchanging processual memory and unpredictability associated with abortions as well as the giant improvements made with medical technology, the ruling of the Roe v. Wade case has led to the future of abortion technology to be in a current state of uncertainty.
-Joshua Manring
References
[1] “In-Clinic ‘Surgical’ Abortion Procedures: What Are They, Who Needs Them?” ABC News, ABC News Network, https://abcnews.go.com/Health/clinic-surgical-abortion-procedures/story?id=87013603.
Shipping mifepristone through the United States Postal Service. [1]
New regulations and bans on abortion have been increasing rapidly in several states since the overturn of Roe v. Wade in 2022. Due to these limitations, interest in Mifepristone by online order and telemarketing has grown. Mifepristone is a medication used for medical abortion in early pregnancies that has become more recently available through the mail in recent years. While the drug is generally considered safe and effective, new regulations and restrictions are attempting to limit its distribution.
When combined with misoprostol, Mifepristone can terminate a pregnancy in the first ten weeks by blocking the progesterone hormone. It is a drug that “The FDA has determined that it is not necessary for the REMS to mandate how providers clinically assess patients for the duration of pregnancy,” making the drug shipment the easiest option. [7]
Medicated abortion makes up about 54% of abortions in the United States [2]. Therefore, many will turn to online ordering for access if that medication is no longer allowed in a specific state. Currently, in states where abortion, both medicated and procedural, has been deemed illegal, access to the pill by mail is still permitted. Although red tape has increased since the overturn of Roe v. Wade.
To limit access, the Food and Drug Administration (FDA) implemented the Risk Evaluation and Mitigation Strategy (REMS). This program required that Mifepristone be only prescribed and dispensed by healthcare providers who have completed the necessary certification process. While this may limit the pill’s access, it does not account for overseas shipments. The FDA then issued a regulation in 2020 that Mifepristone could not be dispensed by mail for fear of complications that would require medical assistance.
Concern of safety over online abortions access. [9]
This restriction has been criticized by reproductive rights advocates, who argue that it puts unnecessary burdens on women seeking medical abortion and can result in delays in care. They say that telemedicine is safe and effective for medical abortion and that the FDA’s restrictions are not based on scientific evidence.
Similarly, in Canada, Mifepristone is only available through a prescription from a healthcare provider and cannot be dispensed by mail. The restrictions on Mifepristone by mail have been criticized as a barrier to accessing safe and effective abortion care, particularly for women living in rural or remote areas.
In contrast, some countries, such as the United Kingdom, have allowed Mifepristone by mail under certain conditions. In the UK, Mifepristone can be prescribed by a healthcare provider, dispensed by a licensed pharmacy or clinic, and then sent by mail to the patient. The use of Mifepristone by mail in the UK has been shown to be safe and effective and has been praised for increasing access to abortion care, particularly for women in rural areas. [6]
As for the postal service, at this time, they “cannot be held criminally liable for conducting their duties by delivering mail that contains medication that can induce abortions” [2]. The postal service has held its ground and will continue its existing practice of delivering the pill. It has stated it will make no efforts to prevent mailers from sending such medications. Therefore, the issue boils down to the pill’s prescriber, provider, and receiver rather than the postal service itself.
However, in 2021 this was challenged in court, and the restrictions were ruled unconstitutional by the supreme court. Many challenged this using the Comstock Act as evidence. This concern was due to the Comstock Act of 1873, which prohibited the delivery of “obscene” items or contraceptives. However, because Mifepristone can be used for other purposes and recipients do not have to claim how they will use the item, neither party involved in the delivery of the pill can be persecuted. [5]
As of today, the clarity of the issue remains foggy; many states are directly attempting to block access to abortion pills and attempting to block access to abortion pills [5] and incriminate providers. The Justice Department still states that it is legally allowed to deliver the pill to states where the procedure is outlawed. Therefore, it is still possible for women to get a legal prescription “via telehealth consultation with a health professional, and then receive the pills through the mail” [3].
The extreme complications and complexity of the issue surrounding mail-order abortion is one that changes day by day. The ability to ship something overnight is a fairly never ability, and rapid developments like these are making the issue more difficult to manage each day. When the issue of state’s rights crosses with the FDA, the supreme court, the post office, and overseas shipments controlling a drug only illegal in certain areas can become messy. As many fight for the right to abortion in their state, I think many will begin to fight for the freedom to mail the pill into their state as this will become more prevalent as more and more states crack down on abortion.
-Molly Weinberg
Works Cited
[1] “Gender & Identity.” The Washington Post, WP Company, https://www.washingtonpost.com/gender-identity/.
[2] Katz, Eric. “The Postal Service Can Continue to Deliver Abortion Pills Anywhere in America, DOJ Says.” Government Executive, Government Executive, 4 Jan. 2023, https://www.govexec.com/management/2023/01/usps-can-continue-deliver-abortion-pills-anywhere-america-doj-says/381441/.
[4] Spencekimball. “Women in States That Ban Abortion Will Still Be Able to Get Abortion Pills Online from Overseas.” CNBC, CNBC, 27 June 2022, https://www.cnbc.com/2022/06/27/women-in-states-that-ban-abortion-will-still-be-able-to-get-abortion-pills-online-from-overseas.html.
[5] “Justice Dept.: Despite Bans, Abortion Pills May Be Mailed to Any State.” The Washington Post, WP Company, 5 Jan. 2023, https://www.washingtonpost.com/national-security/2023/01/04/abortion-pills-mailed-legal/.
[6] Abortion Safety and Use with Normally Prescribed Mifepristone in Canada …https://www.nejm.org/doi/full/10.1056/NEJMsa2109779.
[7] Center for Drug Evaluation and Research. “Questions and Answers on Mifeprex.” U.S. Food and Drug Administration, FDA, https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/questions-and-answers-mifepristone-medical-termination-pregnancy-through-ten-weeks-gestation.
[8] Farley, Robert. “Noem’s Misleading Claim about Safety of Medication Abortion.” FactCheck.org, 12 July 2022, https://www.factcheck.org/2022/07/noems-misleading-claim-about-safety-of-medication-abortion/.
The Pink House (Jackson Women’s Health Organization), the greater Mississippi area’s last abortion clinic, was forced to shut down in the wake of the overturning of Roe v. Wade (NPR).
In their Maternal and Child Health Journal article, Pari Chowdhary, Anna Newton-Levinson, and Roger Rochat reported what abortion providers identified as challenges they face. In order to preserve women’s access to safe abortion procedures in post-Roe America, there needs to be a “steady maternal health workforce,” but the restrictive laws in place in some states have caused regional provider shortages. Those who do provide abortion services regard this “restrictive legislation” as a significant challenge causing domino effects, such as “institutional separation of abortion from other medical services, training unavailability, safety concerns, identity struggles, and marginalization within their profession.” Abortion providers currently face stigma and isolation not only within the environment of healthcare work (their occupational world) but in their lives as well. Although some providers are driven by restrictive laws to practice in states without them, some choose to continue practicing despite challenges because they want to make a difference in areas of high need and to combat disparities in healthcare access… or simply because they have personal ties to the state.
As Selena Simmons-Duffin writes in a 2022 NPR article, doctors who decide to stay in states that have banned abortion find their medical opinions being overridden by laws that they don’t want to risk breaking. Some legislation prohibits abortion aside from cases involving medical exception, but “deciding what cases qualify … can be a difficult judgement call for doctors.” This may lead them to take a ‘better safe than sorry’ approach when it comes to violating these laws, even if it’s the less safe or healthy option for the patient. However, flat-out denying treatment is not the only harmful consequence of these laws– sometimes doctors delay care because they want to ensure they’re not violating legislation. In his address to the American Medical Association’s legislative body, president Dr. Jack Resneck expressed how he “never imagined colleagues would find themselves tracking down hospital attorneys before performing urgent abortions, when minutes count, [or] asking if a 30% chance of maternal death or impending renal failure meet the criteria for the state’s exemptions, or whether they must wait a while longer until their pregnant patient gets even sicker.'”
In other states, abortion procedures are denied even in obvious emergency situations: for example, a woman who’d been profusely bleeding for hours from a miscarriage was not initially treated at an Ohio ER, NPR reported. Additionally, as Springfield News-Leader described, a woman whose water broke at 18 weeks (leaving her at risk for infection) was denied an abortion procedure by hospital doctors because “current Missouri law supersedes our medical judgement.” This hospital is currently under investigation for going against a federal law requiring doctors to treat and stabilize patients during medical emergencies, but this case nevertheless exemplifies how abortion law presents challenges to healthcare providers that may lead them to withhold services for fear of the legal repercussions of offering them, or opting for riskier procedures. For example, a Texas Policy Evaluation Project survey found that “clinicians sometimes avoided standard abortion procedures, opting instead for ‘hysterotomy, a surgical incision into the uterus, because it might not be construed as an abortion.'” Dr. Matthew Wynia, Director of the Center for Bioethics and Humanities at the University of Colorado, says this procedure is “much more dangerous, much more risky– the woman may never have another pregnancy now because you’re trying to avoid being accused of having conducted an abortion.” Doctors don’t want to break the law by performing an abortion, so they put mothers in danger by delaying, or (worse) denying, care. “If the law is wrong and causing you to be involved in harming patients,” Dr. Wynia wrote in his New England Journal editorial, “you do not have to live [within] that law.”
Before Roe v. Wade was first passed in 1973, “there was ‘almost a ‘don’t ask, don’t tell’ kind of silence’ around” abortion providers, according to UC Davis legal historian Mary Ziegler, who specializes in abortion history. By the 1940s, however, abortion had become increasingly criminalized, which led to the formation of “therapeutic abortion committees” in the 1950s, protecting abortion providers from legal repercussions and allowing abortions in certain circumstances (i.e. emergencies). Then, in the 1960s, the focus shifted from navigating around and avoiding anti-abortion legislation to confronting it: doctors started trying to get caught and arrested, so that their cases would get publicized and draw attention to the “vague or unworkable” legal restrictions. However, this is no longer the case. “In the five months [after] the Supreme Court overturned Roe v. Wade, leading medical associations [told] NPR they [weren’t] aware of any health care workers … charged with providing an abortion in violation of these new state laws,” partly because the new laws are so much more extreme. “Now, many of these state laws,” Simmons-Duffin explains, “were written explicitly to criminalize doctors, with penalties that include felony charges, prison time, fines, and the loss of their medical license and livelihoods. The maximum penalty for doctors who violate Texas’s abortion ban is life in prison.” These are very real threats for doctors, since (unfortunately) in the modern political climate, their cases are likely to be lost. “There is no way that I would risk my personal freedom and jail time for providing medical care,” says Indiana-based OB/GYN Dr. Katie McHugh. “I would love to show my children that I am brave in the world, but our society will not allow me to be a civil-disobedient citizen … I would be imprisoned, I would be fined, I would lose my license and I very well could be assassinated for doing that work.” However, there are two methods of disobeying anti-abortion legislation, according to bioethicist Katie Watson, who also serves as professor of law and humanities at Northwestern University’s medical school. The first is civil disobedience, violating legislation “publicly to make a point.” This is obviously the approach that has been taken historically, but in the face of more restrictive legislation there’s been a shift toward “‘covert disobedience,’ which is privately resisting the law.” As Watson explains, “that is when you believe a law is unjust and you do not believe disobeying it in public will change it, but there is an identified other in danger in front of you that you have the resources to help.” Historical examples of covert disobedience include the Underground Railroad or hiding Jews from the Nazis. In the context of abortion providers, this looks like referral systems that send patients to different places to receive abortion care. This allows abortion providers to ensure “patients can still get care without risking their livelihoods and personal freedom.”
Of course, the illegalization of abortion in certain states has deterred some doctors from practicing in those states in the first place. Even if a doctor does not plan to provide abortion care, the abortion bans (laws meant to protect fetuses) present unique liabilities and limits for regular medical practice. Additionally, some doctors don’t want to associate with a state that does not align with their personal values (being pro-choice). This means that these states are at a disadvantage amidst the current reproductive health practitioner shortage– “some prospective OB/GYN candidates won’t even consider opportunities in states with new or pending abortion bans.” In fact, there have been at least 20 instances (according to Tom Florence, president of AMN Healthcare company Merritt Hawkins) where prospective doctors have specifically refused to practice in states where reproductive rights were legally constricted out of fear that “‘…they could be fined or lose their license for doing their jobs.'” Doctors currently being trained are presented with challenges by the overturning of Roe v. Wade, as well — mainstream physicians in support of abortion rights “worry that limits on training for new doctors will undermine recruitment of young talent,” concerned that restrictions will prevent prospective healthcare professionals from reaching their full potential by limiting the services they can offer.
The overturning of Roe v. Wade presents challenges not just for doctors but entire abortion clinics. As Shalina Chatlani writes in her Tennessee Lookout article “Remaining Abortion Clinics Face More Challenges If Abortion Pill Limited by Texas Judge,” clinics across the country have been shut down due to the overturning of Roe v. Wade. For example, Jackson Women’s Health Organization (“The Pink House”), which for years had been the only abortion clinic serving the greater Mississippi area, was forced to shut down following the Supreme Court ruling. Its transformation into a luxury consignment shop has begun– the iconic pink walls have been painted over (there are no longer protesters outside of them); the medical equipment that was once inside, not serving a purpose anymore, has been removed. Many women in Mississippi, as well as other Southern states, are traveling elsewhere to seek abortions, whether via drugs or an in-clinic procedure. However, a federal judge in Texas is deciding on an anti-abortion lawsuit directing the FDA to withdraw approval of mifepristone, a decades-old drug widely used in medical abortion. Medication abortions account for the majority of all abortions in the US, the Guttmacher Institute reports, so the consequences of a ruling in the anti-abortion groups’ favor would definitely be felt. Restrictions on medication abortions are currently most prominent in our area of the country, the southeastern United States, but “the likely immediate impact [of an anti-abortion biased ruling] would be that manufacturers would not be allowed to ship mifepristone anywhere in the United States, and providers would no longer be able to prescribe it.” This would be yet another law that would limit providers, preventing them from providing certain services. This may, as previously stated, deter doctors from working in anti-abortion states– they may follow women who seeking abortion to states in which offering abortion services is legal. However, the immigration of clients to clinics in these states presents those clinics with the challenges of increased demand. Mara Pliskin, patient navigation manager at Planned Parenthood in Illinois, describes it as being “in the trenches.” These clinics are trying to put systems in place to take in this large influx of patients as quickly as possible, as patients may be in dangerous situations, but often end up having to create waitlists (which will grow if medical abortion is restricted).
Chatlani’s article also discusses a challenge faced by abortion advocacy & reproductive justice organization Yellowhammer Fund: after the overturning of Roe v. Wade, the nonprofit not only “had to effectively stop most of its abortion-related services” but were also limited to only providing information already available in the media. The organization’s focus, says deputy director Kelsea McLain, has shifted to their programs that support new parents.
An American Civil Liberties Union article describes TRAP (Targeted Regulations of Abortion Providers) laws, which “require abortion providers to have admitting privileges at local hospitals or require clinics that provide safe, outpatient care to meet the standards of ambulatory surgical centers.” These requirements are challenging, sometimes impossible, to fulfill. Most hospitals won’t admit abortion providers, and the safety of the abortion procedure prevents doctors from meeting the hospital-admit patient threshold. In May 2017 (pre-TRAP), there were 6 states with only one remaining abortion clinic; this number could soon rise to at least 8, and some states could have no abortion clinics at all.
As Max Zahn of ABC News reported, abortion bans have led to financial losses for clinics. His article, “Abortion Clinics in Embattled States Face Another Challenge: Money” focuses on Katie Quinonez, executive director of Women’s Health Center of West Virginia. When the nonprofit faced prosecution under a West Virginia abortion ban from 1882, Quinonez and her coworker called to cancel 60 procedures scheduled for the following 3 weeks, which was “a crushing blow to the nonprofit health center’s financial stability.” As Quinonez points out, clinics’ financial situations are typically already tight, meaning abortion bans are especially detrimental in this regard. Unfortunately, according to clinic officials and reproductive health organizations, the two options now faced by abortion clinics are expensive: either move to a state where abortion is legal, or remain open but stop providing abortions. The latter deprives clinics of a key revenue source (for example, Quinonez reports that abortions accounted for 40% of her clinic’s revenue, a large portion of their $1.6 million annual budget). The former means losing revenue from established patients while gaining moving expenses. Clinic budgets might not be able to handle this, Quinonez worries, because in addition to complying with these regulations, they are depending on low-income patients who often lack insurance, and they themselves lack federal funding (and, in many cases, Medicaid coverage).
Across the country, abortion providers are sticking their necks out in order to fight for what they believe in. Abortion bans present challenges for clinics and doctors who offer these procedures, but providers are able to counter-challenge in three main ways. Mabel Felix, Laurie Sobel, and Alina Salganicoff outline these challenges in their KFF article “Legal Challenges to State Abortion Bans Since the Dobbs Decision.” The first category of challenges is Broad Constitutional, which can be seen in states including Oklahoma, Georgia, Utah, and Ohio and includes claims stating constitutional protections (i.e. liberty; due process; privacy rights) protect abortion rights. Health Care Amendment Challenges argue that state constitution amendments to include rights to healthcare/health insurance decisions include a woman’s right to choose; this category of challenges is seen in states such as Ohio and Wyoming. The final category of challenges to abortion bans is Religious Freedom: arguments that abortion bans “either unduly infringe on … religious exercise or violate state constitutional protections against the establishment of religion” in Wyoming, Indiana, Florida, Kentucky, Utah, and Missouri.
As it did in most areas of our lives, the COVID-19 pandemic (which preceded the overturning of Roe v. Wade) presented many challenges in regards to abortion. In their study “The Impact of COVID-19 on Abortion Providers,” a research team at University of California San Francisco’s ANSIRH (Advancing New Standards In Reproductive Health) program found that the pandemic caused abortion provider shortages, forced clinic closures, “led to increased expenses and reduced revenues,” delayed ability to provide services, and overall disrupted the ‘flow’ of clinics. As previously stated, these types of problems have been exacerbated by Roe v. Wade being overturned: there are practitioner shortages in states that have banned abortion; abortion clinics have experienced financial strain that, in some cases, forces them to shut down; there’s obviously an inability to provide abortion services without legal consequences, and the field of women’s healthcare has been drastically altered.
Chowdhary, Pari, et al. “‘No One Does This For The Money Or Lifestyle’: Abortion Providers’ Perspectives on Factors Affecting Workforce Recruitment and Retention in the Southern United States.” Maternal and Child Health Journal, vol. 26, no. 6, 2022, pp. 1350–1357., https://doi.org/10.1007/s10995-021-03338-6.
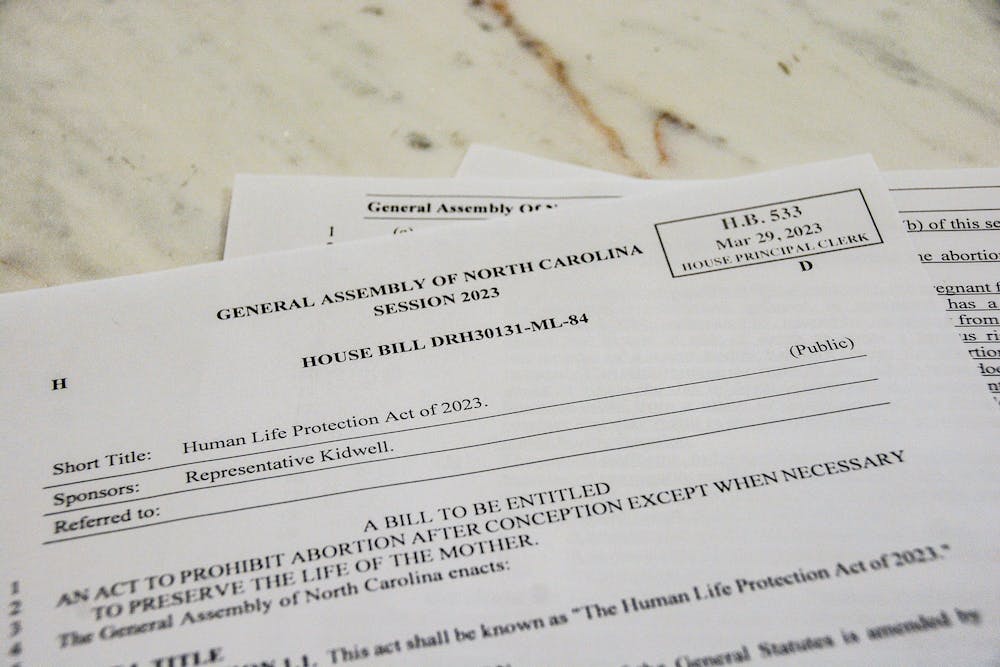
Representative Keith Kidwell (R-Beaufort) introduced H.B. 533 to the NC State House on March 29th, 2023. [6]
Since June 2022’s landmark Dobbs v. Jackson decision returned regulatory power of abortion to the individual states, North Carolina has been embroiled in a hugely partisan divide over the future of abortion in the state. Represented by the state’s Democratic and Republican Parties, led by Governor Roy Cooper and NC House Speaker Tim Moore respectively, North Carolina’s political battleground over abortion and reproductive rights typifies the contentious and ever-shifting nature of this debate throughout the United States as a whole.
On July 6th, 2022, just a week and a half after the Dobbs decision, Governor Roy Cooper issued an executive order to protect access to reproductive health care in North Carolina. This order, which was effective immediately upon its release, explicitly protects all reproductive health services “including, but not limited to, services relating to pregnancy, contraception, or the termination of a pregnancy” [2]. However, despite Cooper’s efforts, North Carolina has made other moves to restrict abortion. On August 17th, 2022, District Judge William Osteen lifted an injunction on an NC law that bans abortion past 20 weeks. While Osteen had originally blocked this law from enforcement in 2019, he cited Dobbs as justification for reinstating the ban, as “there is now no constitutional right to a pre-viability abortion, thus depriving the injunction of any constitutional basis” [5]. Where Speaker Tim Moore lauded this decision as “a ruling that upholds the law”, Cooper publicly criticized it, stating that “denying women necessary medical care in extreme and threatening situations, even if rare, is fundamentally wrong” [5]. As North Carolina law currently stands, abortion is legal up to 20 weeks.
In the past month, NC Republican lawmakers gained increasing traction to further abortion prohibitions. Previously, the NC GOP publicly discussed options for banning abortions either after the first trimester or based on fetal cardiac activity in a so-called “heartbeat bill” [4]. However, on March 29th, 2023, Representative Kidwell, R-Beaufort, filed HB-533, or “Human Life Protection Act” which would “prohibit abortion after conception except when necessary to preserve the life of the mother” [4]. This bill is significantly more restrictive than the previously discussed options, cutting access to abortion with few exceptions and at a criminal cost to health providers. At the time that HB-533 was introduced, it was expected to face gubernatorial veto, which could not be overruled by the Republican Party, and was expected to act as a symbolic gateway to pave the way for similar, but slightly less restrictive legislation surrounding abortion.
The NC State Capitol in Raleigh, NC. [3]
However, on March 30th, the tides shifted for the NC GOP as State Representative Tricia Cotham announced she would no longer be a Democrat, stating that “The modern-day Democratic Party has become unrecognizable to me and to so many others throughout this state and this country” [1]. Representing the 112th District in Mecklenburg County, Representative Cotham has historically been a reliable Democratic vote in the State House. In fact, she once shared her personal experience with abortion on the House floor, “accusing Republican lawmakers of ‘wanting to play doctor’” [1]. Regardless, Cotham’s defection allowed the Republican Party to secure a veto-proof supermajority in both the State House and Senate, which could help to push bills like HB-533 that Governor Cooper would have vetoed into North Carolina law. Since Governor Cooper took office in 2017, he has vetoed over 75 Republican-sponsored bills, so this power shift is sure to have lasting ramifications in the NC legislature [1].
Despite these shifting restrictions, North Carolina experienced a 37% increase in abortions between April and August 2022, which is the largest surge in care experienced by any state sincethe fall of Roe v. Wade [2]. People seeking reproductive choice in neighboring states like Tennessee have travelled to abortion clinics in Chapel Hill, Charlotte, and Ashville, accounting for the uptick in provided abortions and subsequent pushback from protestors. As a reaction to this increased activity, some more rural counties throughout NC have even gone as far as to declare themselves symbolic “sanctuaries for the unborn” to express their opposition to this stark increase [2]. A February 2023 poll from Meredith College reported that the divide in public opinion is “entirely partisan”, as over 3/4ths of Democrats wish to keep or expand NC’s current protections, while 60% of Republicans wish to further restrict access. This fervent, partisan divide regarding reproductive care across the state’s constituents reflects the similar conflict at the governmental level.
The legal status of abortion in North Carolina is a rapidly shifting political debate, serving as a representative case study in memory politics in the United States overall. The centrality of abortion to North Carolina’s political landscape itself shows how the Ramifications of Roe and Dobbs are only just beginning to surface. The speed at which the NC legislature has presented restrictive legislation and secured supermajority in voting demonstrates the processual way lawmakers interpret and reinterpret official memory through law. As Americans, and specifically as North Carolinians, we are experiencing events in our history every day that have the power to forever change not only our rights, but the way we conceptualize abortion and reproductive health as a whole.
[3] Loanes, Ellen. “A North Carolina Democrat left the party — and shifted the balance of power”. Vox News. 09 April 2023. https://www.vox.com/2023/4/9/23674306/north-carolina-tricia-cotham-republican-party-switch. Accessed 19 April 2023.
For women, the entirety of their history in the United States revolves around one thing: their fight for freedom in multiple avenues such as their body and their intellect. When women were presented the supreme court case of Roe v. Wade, which is a landmark case that established a women’s right to abortion, their entire future changed. What did this change look like? Women across the country found not only a newfound liberty over their own body, but they also discovered new feminist ideals within themselves that created a beautiful connection between their inner and outer freedom. When the case was finalized and they were given the right to choose, women proclaimed their new freedom through more political participation, reevaluating the cultural and social context of the decision, and identifying how the decision changed their access to hospital resources post Roe v. Wade.
When the United States decided to make the decision to make abortion legal, women channeled their inner feminism and let it be seen through new political participation, especially as, even to this day, there will always be backlash from parts of the community. In a journal from Greenhouse and Siegel they examine how, during the beginning of the feminist movement in the 1960s, women didn’t originally understand that during their fight for equal education and pay, abortion actually fit into the puzzle. However, as time went on and the 1960s came to an end, women began to realize that child bearing is something that they too should have freedom over. When women discovered this, they began their fight for abortion freedom until they won with Roe v. Wade decision of 1973. When Roe v. Wade was first being discussed, there was a party realignment that occurred due to the Democrats siding with women’s rights and the Republicans trying to get the attention of those who were “pro-life” such as the catholic population [2]. With this and the party polarization, many women found themselves sticking to their beliefs and thus becoming more politically active as a whole. The inclusion of women in politics would be forever changed and the memory of the impactful court case decision did not go unnoticed. Looking forward to today, women are more active than ever, especially in women’s rights related issues such as abortion and equal pay in marches and rallies as a result. Roe v. Wade was a decision that gave women a new confidence in their political participation, and it had an effect that made women realize that their entire body is their own, and it is not up to the government to control that for them.
There is an incredibly intricate relationship between freedom and feminism and what it looks like when evaluating the cultural and social context of Roe v. Wade. When the case first concluded, women were ecstatic to finally have the right to have an abortion, but they failed to realize the other implications that came with this newfound freedom. While yes, abortion was now legal, accessibility became an issue. In “Reconceiving Abortion: Medical Practice, Women’s Access, and Feminist Politics before and after ‘Roe v. Wade” by Schoen, it is explained following Roe v. Wade, the narrative changed from being about abortion itself and instead access. During this time, it was mostly those in more metropolitan areas and available to the middle and high class individuals that populated them [3]. With this and the narrative shift, women continued their feminist fight, but in a different light. In evaluating the social and cultural context, women not only looked at where their place was in society, and where they could make a difference. There was a clear race and class divide in access, and the community of women who fought for Roe v. Wade in the first place began their fight for access.
Similar to the last point regarding accessibility, the ways in which hospitals functioned around abortion changed following the decision which, in turn, gave women more freedom. In a study done by Bond and Johnson, they found that “almost half of the hospitals (47 percent) changed their abortion policies after 1973. A small number (5 percent) restricted their services, but a much larger number (42 percent) expanded their services” [1]. For most hospitals, this change evolved from providing only therapeutic abortions to elective, which means that hospitals were allowing women to choose abortions if they wanted, not only if they had to. This change sparked a whole new life for women in America. Because of these changes, a woman could walk into a hospital, requesting an abortion, and receive one without any backlash. This change in history, whether women of today think of it or not, changed society’s cultural memory revolving around the decision. In today’s society, before the current court case, women can walk into an office or abortion clinic and feel no discomfort from the staff. Freedom was something that was hard for many women to completely feel in a hospital setting back then, but with policy change came feministic freedom that would forever change their experience.
The intricate relationship between feminism and freedom after Roe V. Wade is one that requires multiple outlooks and understandings as with more freedom comes more difficulties. While political participation changed, and has continued to evolve, setbacks such as accessibility kept full freedom from occurring for some time. Women in the 1970’s and the women of today share a lot in common: they embody their feminism with a drive for full freedom as they fight for abortion rights, equal pay, and accessibility to resources despite class or race. The ways in which women’s rights will be remembered in memory started with this monumental case, and will likely never end. Roe v. Wade was a life-altering case for women across not only America but the world, and its implications continue to drive women to work for a better tomorrow for freedom.
– Courtland Bartosik
Works Cited
[1]Bond, Jon R., and Charles A. Johnson. “Implementing a Permissive Policy: Hospital Abortion Services after Roe v. Wade.” American Journal of Political Science, vol. 26, no. 1, 1982, pp. 1–24. JSTOR, https://doi.org/10.2307/2110836. Accessed 11 Apr. 2023.
[2]Greenhouse, Linda, and Reva B. Siegel. “Before (and After) Roe v. Wade: New Questions About Backlash.” The Yale Law Journal, vol. 120, no. 8, 2011, pp. 2028–87. JSTOR, http://www.jstor.org/stable/41149586. Accessed 11 Apr. 2023.
[3]Schoen, Johanna. “Reconceiving Abortion: Medical Practice, Women’s Access, and Feminist Politics before and after ‘Roe v. Wade.’” Feminist Studies, vol. 26, no. 2, 2000, pp. 349–76. JSTOR, https://doi.org/10.2307/3178538. Accessed 11 Apr. 2023.
Abortion and women’s reproductive rights have been a topic of contention over the last half-century. Organizations around the world have been formed in both support and contestation of these rights. As the 50th anniversary of the historic Roe V. Wade supreme court case was approached and ultimately overturned, it is important to reflect on the way this memory was celebrated and the processual way this celebration changed. During the 1950s and 1960s, illegal abortions were found to be extremely common and usually entailed dangerous and life-threatening procedures. One survey found that” the number of illegal abortions in the 1950s and 1960s ranged from 200,000 to 1.2 million per year … extrapolating from data from North Carolina, concluded that an estimated 829,000 illegal or self-induced abortions occurred in 1967″,[1] which notes how illegal and dangerous abortions were extremely common in the United States. These shocking statistics peaked the interests of many groups across the country and led to widespread support for the legalization of abortions
A leading organization in this support was a group of feminists called the “Redstockings”. The group was formed by Ellen Willis and Shulamith Firestone in 1969 and consisted mostly of Jewish women whose goal was to combat the legal ban on abortions, later expanding to fight all oppression, using what was considered “radical” approaches.[2] This group would show up to legal hearings and other large gatherings, seemingly out of nowhere, and protest legislation that put a ban on abortions. These radical techniques would become what is known as “raps” and are still used by many political protesting organizations in the 21st century [3]. The Redstockings led a revolution in the way people rallied and protested ideas. Eventually, their work paid off in 1973 when the supreme court ruled that the right to an abortion was supported by the U.S. Constitution in Roe V. Wade.
Symbol of the Redstockings liberation movement, the red stands for the “radical” actions the group takes to combat sexism
This led to many members celebrating this historic court case by organizing marches and sharing personal stories about their own experiences with abortions. This celebration became a longstanding tradition and a way of commemorating this specific moment. The Redstockings and their initial actions have set the standard for reflecting upon the memory of this supreme court decision. However, now that Roe V. Wade has been overturned by the decision in Dobbs V. Jackson Women’s Health Organization in 2022, the 50th-anniversary commemoration of women’s federal rights to abortions has been thwarted. Individuals can no longer celebrate this federal right and must change how they view the memory of Roe V. Wade and those who fought for it to be passed.
Interview with Joyce Chediac, a former member of the Redstockings, that analyzes the impact of the overturning of Roe V. Wade.
This means the Redstockings must be analyzed in a different light than just the traditions they have started. They must be looked at in how they began their movement and where their cause began. The first real action of this group can be traced back to February 13th, 1969 in Albany, New York. On this day, a group of members of the Redstockings gathered at the New York state house and disrupted a public hearing on abortion. The group appeared at the hearing and started chanting and demanding that the leading council hear their voices and concerns. After this, the hearing was moved to a private area where only council members could speak on the topic. Some of the Redstockings were able to enter this area and found that out of the 15 council members, only one was a woman. This led to many members gathering outside the doors and eventually causing enough of a commotion to break up the hearing. This was the first case of the Redstockings pushing against the legal ban on abortion and retaliating against lawmakers.
A group of Redstocking members rallies outside of a private hearing on abortion in the New York State House on February 13th, 1969
Due to the recent overturning of Roe V. Wade, a process has started in which the memory of this event has become one that is being extensively looked at. Roe V. Wade can no longer be commemorated and celebrated as the Redstockings did after 1973. Instead, groups are starting to adopt this retaliation seen in 1969 and push against lawmakers and other individuals that thwarted the 50th anniversary of Roe V. Wade. It is a way in which memory is both a particular idea and a changing process that never stays static. Individuals have now started to, again, fight for the right to an abortion as seen on June 24th, 2022 at the Wisconsin State Capitol. A group of pro-abortion activists gathered at the steps of the capital and began protesting the decision to overturn Roe V. Wade. These individuals protested for hours with one protester stating I think it’s ridiculous that it’s 2022 and I still have to fight for my reproductive rights, “I mean, when have men ever had any of their rights in general questioned?” [4] The memory of the Redstockings has been used here to bring upon action like in their “raps” protests and turn to the ideas of feminist pushback against the oppression of women. It is a continuation of the memory that started in 1969 in which almost 50 years after the initial legalization of abortions, women a reliving the same lives the Redstocking members did.
Protestors outside of the Wisconson State capital on June 24th, 2022
One challenge of refining your selections for our Remembering Roe memory project is to anchor your theme topic of particular memory.
The task of your research at this stage is to focus your inquiry to locate the particular anchor that embodies its significance and serves a central site/vehicle through which the impact of Roe v. Wade and the history and practices it represents has been remembered.
This might seem too narrow but a defined focus will allow the specificity of your selected research site to serve as a prism for revealing the issues of your larger topic in an applied way. It will also empower you with a more targeted process of research. To do this you should read more broadly in your topic, take notes, and develop a list of increasingly focused keywords – revealed to you in your research — than can unlock other instances of how your memory circulates.
Find useable particulars within your larger memory topic by defining its focus into specific instances and see which ones provide the most telling angles for more focused analysis.
Don’t rely only on search engines to find materials for your site!!
Define a varied list of specific keywords for your site and use them in different combinations to find useful materials in the databases on UNC’s library webpage and begin with an Article+ search. https://library.unc.edu/find/articles/
Look up, using your specific keywords, how your site has been covered in the media (with what different keywords) by seeking out local newspapers in the America’s News database which can be searched at the State level. Use this database (but you will need very focused keywords)!
Use different combinations of your focused keywords to search in Google scholar: http://scholar.google.com/ when you find a good source, click on the “Cited by” link to see more recent research that used this article
Full-text databases beyond the ones mentioned above that might prove especially useful include Academic Search Premier, Proquest Central, OCLC Firstsearch, and Proquest Dissertations and Thesis, as well as JSTOR and Project Muse. You can find links to these on the right side of this page. Check out the databases under Women’s and Gender Studies.
Seek out visual, sound, and multimedia representations of your topic and site.
What important contexts do you need to consider to be able to interpret your “site”? (For example, when did it originate and out of what previous memories? Who established it, invented it, and belongs for it? How is it maintained? Who accesses it and how is it used? Who benefits from it? Why has it become popular and representative?)
What kind of conflict and significance is represented by your “site”?
It will be key to argue in your research post how your site is connected to Roe v. Wade and serves as a vehicle for the cultural memories associated with it.
Look for how your “site” may have served as a rally point around which other memory work has accreted and ways that your site has circulated through and influenced other spaces and forms of memory. A measure of the impact and importance of a “site” is how it circulates in popular reference and expression.
Think of how your site meets Zelizer’s premises of being material, particular/universal, unpredictable, processual, useable, and partial (and Schudson’s distortions) and consider how your site embodies these aspects of memory as well as other concepts from our course.





:max_bytes(150000):strip_icc()/license-shutterstock_178095647z-56cddde63df78cfb37a34ded.jpg)

