Five years ago I could not have told you what “public health” was…because I had never even heard the term before. Also, I knew absolutely nothing about cervical cancer before this summer, but now I am working with the Center for AIDS Research (CFAR) on a clinical trial for a pre-cervical cancer treatment: “ACT II: Acceptability and Feasibility of Combination Treatment for Cervical Precancer among South African Women Living with HIV“.

The clinical trial is based in South Africa, but I am working in Chapel Hill with my preceptor (my direct superior/mentor), Dr. Jessica Keys, to build a database on a website called Research Electronic Data Capture (REDCap), a secure survey-building software. What is a secure survey-building software? It is difficult to explain why those adjectives are important and what they mean, but I can only give a brief explanation. REDCap is used to store information such as medication taken by trial participants, symptoms after taking the precancer treatment, and diagnostics/vitals recorded during the trial to monitor the health of the participants. And REDCap is one of many services that can create surveys (such as Qualtrics or SurveyMonkey), but it is one of the most useful because it provides many security measures to prevent breaches of sensitive medical information. Before I could even look at the surveys I had to complete a series of short online quizzes/readings to gain approval into the study. Since gaining approval, I have been translating surveys that were made beforehand into digital versions on REDCap. So, I am essentially taking surveys that are on paper and copying them so that the researchers in the clinical trial can store the information online.
My first expectation for the practicum is to learn biostatistics-related skills such as how to prepare for a clinical trial, how to properly create surveys or other methods of organizing patient information, and possibly learn more about how to analyze large data sets efficiently if time permits. An important thing to know about me is that I went straight from undergrad to this grad program, so my second expectation for this practicum is to develop the professional skills that most other students developed through full time jobs like clear communication in different mediums and maintaining punctuality of assignments and meetings. So far, the practicum has exceeded my expectations.
My first task was to gain IRB approval to join the study and that process was tedious, but necessary for the overall goal of making sure that research is ethical. For example, I had to read about the issues that could lead to unethical research such as conflicts of interest and insecure health records. Luckily, I won’t need to see any patient information during my practicum so there won’t be any worry about confidentiality or data security.
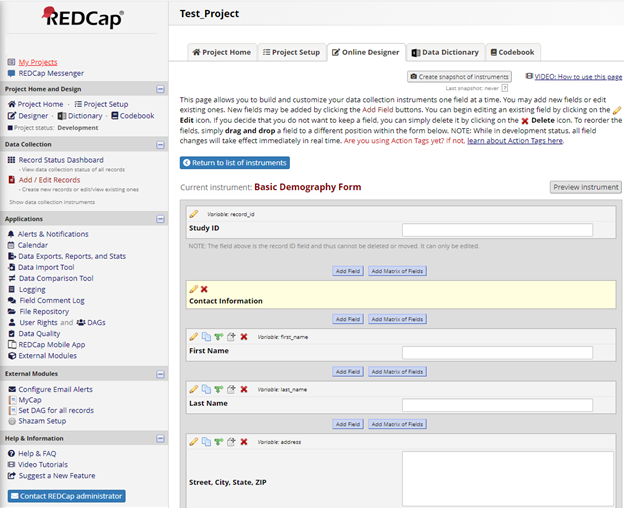
After gaining entry to the study, I have been learning how to use REDCap and gaining tips from my preceptor on the best methods of creating digital surveys to help the research team and analysts do their jobs. Honestly, using REDCap was simple after I watched a few training videos, but the difficult part of building surveys is completing all the behind-the-scenes brainstorming that is necessary to create a high-quality survey. The first objective for building a good survey is to anticipate all the possible answer choices that a participant could give. Related to that is the necessity of providing space to explain any answers that are not popular or anticipated (i.e. “Other, specify:”). Those two objectives may seem obvious but are easy to overlook in the process of creating a survey. The third objective is to raise questions about the quality of the surveys such as: “Are the electronic surveys intuitive for the investigators who are collecting data?” or “Are there any questions that are poorly worded or difficult to translate to the electronic format?” The final objective is to increase the efficiency of communication between the creation of the survey, to collection of the data, and finally to analysis of the survey answers after the participants terminate their participation. Given these four objectives, the summation of my job this summer is to accommodate the collection of information during the trial and prepare for the summation of that information after the trial is over.

Given the position of my work along the timeline of the clinical trial (between collection of the data and analysis of that information), it is important to think about all the ways that data analysis can be made easier for whoever is looking at the results of the surveys. All the coding within the electronic surveys must be intuitive and a spreadsheet should be provided that explains how the electronic versions of the surveys match the paper surveys that were given to me.
When I am not creating surveys on my laptop (usually at Open Eye Café or Weaver Street Market) I am engaged in two other “jobs”! First, I am working part time as a barista at Joe Van Gogh Cafe, which allows me to step away from my work and make some money on the side (around 18 hours a week). Second, I am taking night classes to become an Emergency Medical Technician (EMT) by the end of the summer (around 16 hours of lectures a week). Ultimately, my career goal is to become a nurse practitioner, so my experiences in public health and emergency medical services (EMS) will prepare me for my dream of practicing medicine while simultaneously building more equitable communities.
To recap, the practicum is showing me how clinical trials function internally and is indirectly teaching me about data collection. Also, my role in the clinical trial will give me the chance to meet the researchers who are leading the clinical trial in South Africa. On top of that, I will be busy with my other two jobs as a barista and an EMT. Yet, everything I am doing is leading to my goal of improving life for as many people as I can.
-Ryan