
In human-centered design work, we expect the unexpected, quickly adapt our plan when needed, and fail fast – meaning we quickly realize what doesn’t work and pivot to something that might work better. My work this summer has provided valuable insight into the real [public health] work application of human-centered design, providing valuable lessons in adaptability, creativity and teamwork.
As a refresher, I am working with YLabs, a global design and research organization working to improve health and economic opportunity for young people aged 10–24 years. For most of the summer, I’ve been working on a project called Ask Frankie. Ask Frankie is a platform that supports young people to make informed decisions about their sexual health and wellness through tailored digitally-based decision-support tools and seamless connection to the sexual health products and services they need most. For the first portion of my practicum, I led about 25 expert interviews with a variety of stakeholders, from OBGYNs and leaders of youth-serving organizations to Instagram-based sex education influencers and school-based sex educators.
One of my deliverables was a synthesis of my expert interviews. Some key insights from these interviews include:
- Youth don’t understand how to use health insurance to pay for sexual and reproductive healthcare, especially if they’re on their parents’ insurance.
- Youth in the Central Valley struggle to access youth-friendly healthcare services close to where they live, while maintaining their confidentiality.
- School-based sex education is inadequate and highly variable. Youth aren’t given the tools or knowledge to navigate queer sex, identity exploration, boundaries, and safe sex.
- Youth turn to social media (TikTok, Twitch, Discord, Reddit) and each other to learn about sexual health and wellness and troubleshoot their needs.
- Youth struggle to manage their mental health, and seek out care for a physical ailment, when the underlying issue is psychosocial or emotional.
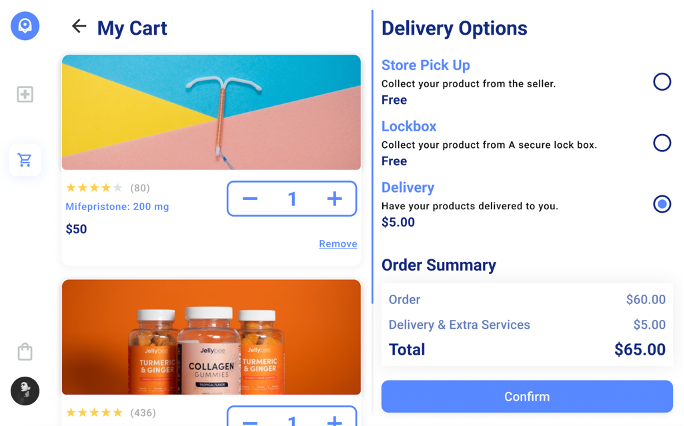
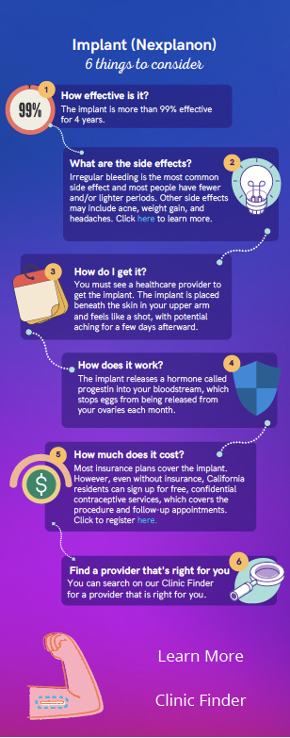
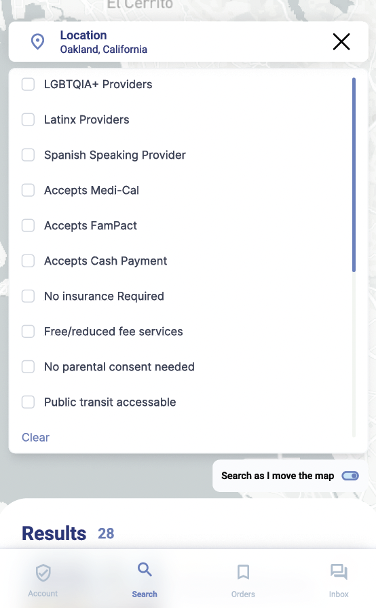
Once I was able to synthesize those data, we were able to use many of those insights to inform the development of rough prototypes of products that might be most helpful to youth we’re working with to develop Ask Frankie. These prototypes, or rough sketches, included a situation-based decision tool, a healthcare service finder, and an online shop for contraceptive products. I was able to apply my knowledge of adolescent and youth sexual and reproductive health (AYSRH) and contribute to rough prototypes meant to be tested out with young people in co-design sessions in the Bay Area and Central Valley of California.
Here are some of the rough prototypes I helped create:
Remember how I said that, in human-centered design work, we expect the unexpected? Well, about a week before I was due to fly out to California for in-person field work, leading co-design and rough prototyping feedback sessions with youth, I broke my foot and had to have surgery. As a result, I could no longer travel to California to complete the last portion of my practicum as planned. This was a major inconvenience both for myself and for the Ask Frankie project. While I recovered, the Ask Frankie team had to quickly adapt and find someone to take my place in the research team. Luckily a colleague was able to fill in, and I was able to give my time to another project looking at male contraception in high income countries.
My work on the male contraception project has been fascinating, and quite a change from exploring the sexual health and wellness needs of youth in California. I got to play with a mixed-method data set of 3,549 adults ages 18-50 from the US, UK, Canada, Germany, Switzerland, France and Spain. The data set examined contraceptive preferences and opinions toward the development of novel male contraceptive options, beyond the market’s current options of condoms and vasectomy. The report is still being drafted, but I hope to be able to direct folks to the report when it is available by the client. It’ll be a fascinating read! Thanks for reading! I am looking forward to the second year of my MPH and being able to walk again!
Zach